
Have you ever woken up in the middle of the night with a shocking sensation of numbness or tingling in your hand? You shake your hand like you’re trying to reset a dead battery, hoping the feeling will return. If this sounds familiar, you might be dealing with Carpal Tunnel Syndrome, also known as CTS. It is the most common upper extremity nerve compression syndrome, where the median nerve gets squeezed at the wrist. It affects roughly 10% of the US population, but it’s not just a statistic-it’s a daily struggle for millions who find themselves dropping keys, struggling with buttons, or unable to grip a coffee mug without pain.
Understanding the Anatomy of Pain
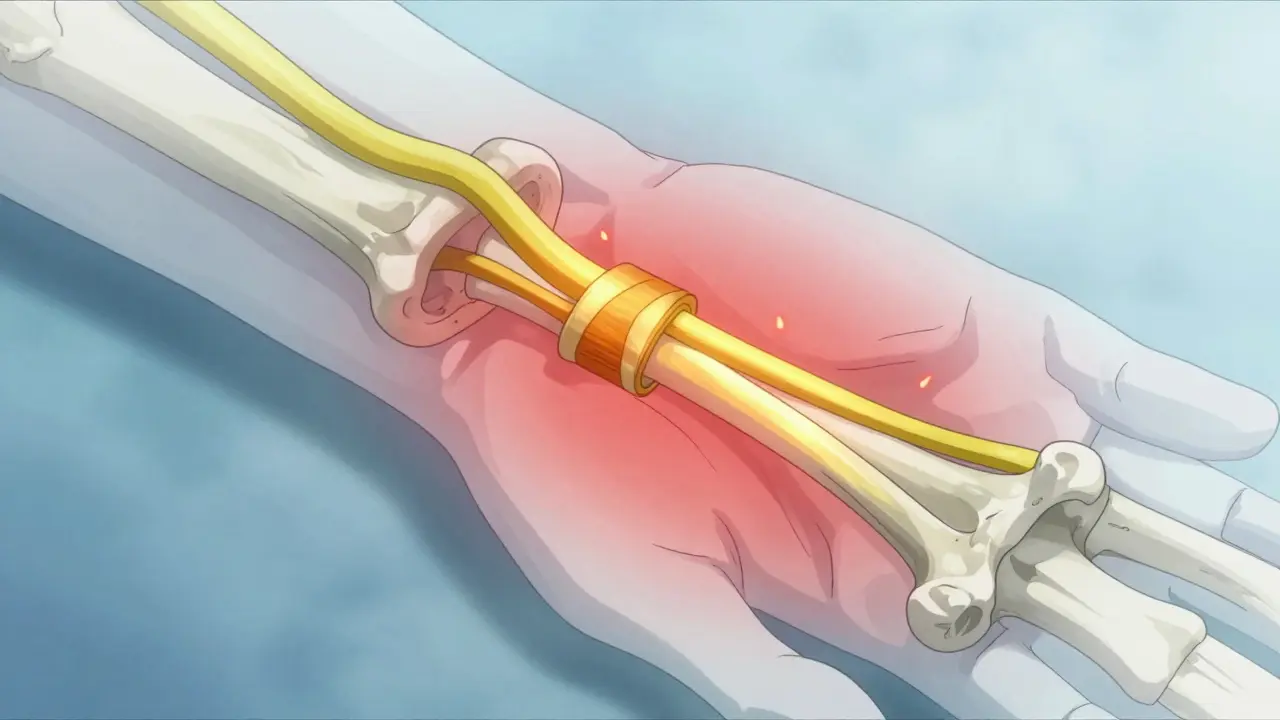
To understand why your hand hurts, you need to look at what’s happening inside your wrist. Imagine a narrow tunnel formed by eight small bones (carpal bones) on the bottom and a tough band of tissue called the transverse carpal ligament on top. Inside this tight space, nine flexor tendons that bend your fingers share room with one critical structure: the median nerve.
The median nerve provides sensation to your thumb, index finger, middle finger, and half of your ring finger. When inflammation occurs-due to repetitive motion, injury, or underlying health conditions-the pressure inside this tunnel rises. This elevated pressure cuts off blood flow to the nerve, causing swelling and eventually damaging the nerve’s protective coating (myelin). According to clinical guidelines from the Journal of Orthopaedic & Sports Physical Therapy (JOSPT), this cycle of increased pressure and impaired microcirculation can lead to irreversible damage if left untreated.
You might wonder why women are three times more likely to develop CTS than men. The answer lies in anatomy; women generally have smaller carpal tunnels, leaving less room for swelling before the nerve gets compressed. Additionally, hormonal changes during pregnancy or menopause can cause fluid retention, further squeezing the already tight space.
Recognizing the Symptoms Early
Carpal Tunnel Syndrome doesn’t hit all at once. It progresses through stages, and catching it early is crucial for avoiding permanent damage. Here is how the symptoms typically evolve:
- Mild Stage: You experience intermittent numbness or tingling, mostly at night. During the day, your hand feels normal between episodes. Shaking your hand usually brings relief quickly.
- Moderate Stage: Symptoms start creeping into daytime activities. You might feel constant tingling or burning sensations. Your grip strength begins to weaken, making tasks like opening jars or turning doorknobs difficult.
- Severe Stage: This is the danger zone. You may experience permanent sensory loss and noticeable muscle weakness in the thumb area (thenar eminence). At this stage, the muscles may actually shrink (atrophy), which is a sign of significant nerve compromise.
If you notice clumsiness-like dropping objects frequently-or if your thumb muscles look flatter compared to your other hand, you need to see a doctor immediately. These are late signs indicating that the median nerve is severely compromised.
Diagnosis: More Than Just a Guess
Many people assume they have CTS because their hands hurt, but diagnosis requires specific testing. Doctors don’t just guess; they use a combination of physical exams and diagnostic tools to confirm the condition.
During a physical exam, a clinician might perform the Phalen test, where you press your knuckles together for 60 seconds to reproduce symptoms, or the Tinel sign, tapping over the median nerve to elicit tingling. They will also check your dexterity using tests like the Purdue Pegboard Test and measure your grip strength objectively.
When physical signs are unclear, doctors turn to electrodiagnostic studies. Nerve conduction studies (NCS) and electromyography (EMG) remain the gold standard for confirming CTS. A median sensory latency greater than 3.7 milliseconds across the carpal tunnel is a key indicator. However, recent research suggests that high-resolution ultrasound is becoming a powerful alternative. An ultrasound showing a nerve cross-sectional area larger than 12mm² at the pisiform level has a 92% sensitivity for detecting CTS, potentially reducing the need for invasive nerve tests.
Conservative Treatments: First-Line Defense
For mild to moderate cases, surgery is rarely the first option. Conservative management is highly effective, especially if started early. In fact, patients who receive comprehensive conservative care within the first 10 months of symptom onset have a 75% success rate, compared to only 35% for those waiting longer.
- Nighttime Wrist Splinting: This is the cornerstone of non-surgical treatment. Wearing a rigid splint that keeps your wrist in a neutral position (0-10 degrees extension) prevents the bending that increases pressure in the carpal tunnel. Studies show that consistent nighttime use for 4-6 weeks improves symptoms in 60-70% of patients. Make sure you wear it every night for at least 6-8 hours.
- Nerve Gliding Exercises: These specific movements help the median nerve slide smoothly through the carpal tunnel rather than getting stuck. A physical therapist can teach you these exercises to maintain nerve mobility.
- Activity Modification: Identify and avoid positions that aggravate your symptoms, particularly keeping your wrist bent beyond 30 degrees for long periods. Ergonomic adjustments at your workstation, such as adjusting keyboard height or using a vertical mouse, can make a huge difference.
- Corticosteroid Injections: If splinting isn’t enough, a corticosteroid injection can reduce inflammation and provide temporary relief. About 70% of patients experience significant improvement for 3-6 months after an injection. This can buy you time to heal or help determine if surgery is truly necessary.

Surgical Options: When Conservative Care Fails
If you’ve tried conservative treatments for 6-8 weeks with no relief, or if you already have muscle weakness and atrophy, surgery is likely the next step. Carpal tunnel release surgery aims to cut the transverse carpal ligament, relieving pressure on the median nerve. There are two main approaches:
| Feature | Open Release | Endoscopic Release |
|---|---|---|
| Incision Size | Larger incision over the palm | One or two tiny incisions |
| Recovery Time | Standard recovery; full duty in 6-8 weeks | Faster recovery; return to work 2-3 weeks sooner |
| Pain Level | More postoperative pain initially | Less postoperative pain (up to 40% less) |
| Success Rate | 90-95% | 90-95% |
| Cost | Lower upfront cost | 15-20% higher due to specialized equipment |
Both methods have similar long-term success rates of 90-95%. However, endoscopic release often allows for a quicker return to light duty work. Newer techniques, like the FDA-approved ultrasound-guided percutaneous release (SX-One MicroKnife), offer even faster recovery with significantly less pain. Despite the benefits, surgery does carry risks. Pillar pain-aching in the thenar or hypothenar eminence-is common, affecting 15-30% of patients during the first few months. Scar tenderness occurs in 5-10% of cases, and serious nerve injury is rare (0.5-1%).
Prevention and Long-Term Management
While you can’t always prevent CTS, especially if genetics play a role, you can significantly reduce your risk. Occupational factors are major contributors. Manufacturing, healthcare, and food service workers face the highest risk due to repetitive motions. Following OSHA ergonomic guidelines, taking frequent breaks, and varying your tasks can help keep pressure low in the carpal tunnel.
If you have underlying conditions like diabetes, rheumatoid arthritis, or thyroid disorders, managing these health issues is critical, as they increase the likelihood of nerve compression. Regular hand stretches and maintaining a healthy weight also contribute to better nerve health.
Remember, early action is your best friend. Ignoring the tingling until it becomes constant pain or weakness leads to more complex treatments and longer recovery times. Whether you choose splinting, injections, or surgery, the goal is the same: to restore function and get your life back without the shock of numbness waking you up at night.
How long does it take to recover from carpal tunnel surgery?
Recovery varies by individual and surgical method. Most patients return to light duty work within 2-3 weeks after open release surgery. Endoscopic release may allow for a return to work 2-3 weeks sooner. Full recovery and resolution of all symptoms can take 3-6 months. Those in manual labor jobs may need 10-12 weeks of modified duty.
Can carpal tunnel syndrome go away on its own?
Mild cases may improve with rest and activity modification, but CTS rarely resolves completely without intervention. Without treatment, the compression on the median nerve can worsen, leading to permanent nerve damage and muscle weakness. Early treatment with splinting or therapy is recommended to prevent progression.
What is the best sleeping position for carpal tunnel syndrome?
The best position is with your wrists in a neutral, straight alignment. Many people naturally bend their wrists while sleeping, which increases pressure in the carpal tunnel. Wearing a nighttime wrist splint helps maintain this neutral position, preventing the flexion that triggers symptoms and numbness.
Does carpal tunnel syndrome affect both hands?
Yes, CTS can affect one or both hands. It is bilateral in about 50% of cases. While it often starts in the dominant hand due to repetitive use, systemic factors like diabetes or pregnancy can cause simultaneous symptoms in both wrists.
When should I see a doctor for carpal tunnel symptoms?
You should see a doctor if nighttime numbness persists for more than a few weeks, if you experience daytime tingling, or if you notice weakness in your grip or clumsiness when handling objects. Early diagnosis prevents permanent nerve damage and expands your treatment options.





