When you're on warfarin, your body is walking a tightrope. Too much blood thinning? You risk dangerous bleeding. Too little? You could get a clot. And the thing that tips this balance more than anything else isn't your genetics, your liver, or even your dose-it's what you eat. Specifically, vitamin K. If you're trying to keep your INR steady, understanding vitamin K foods and how they interact with warfarin isn't just helpful-it's life-saving.
How Warfarin and Vitamin K Work Against Each Other
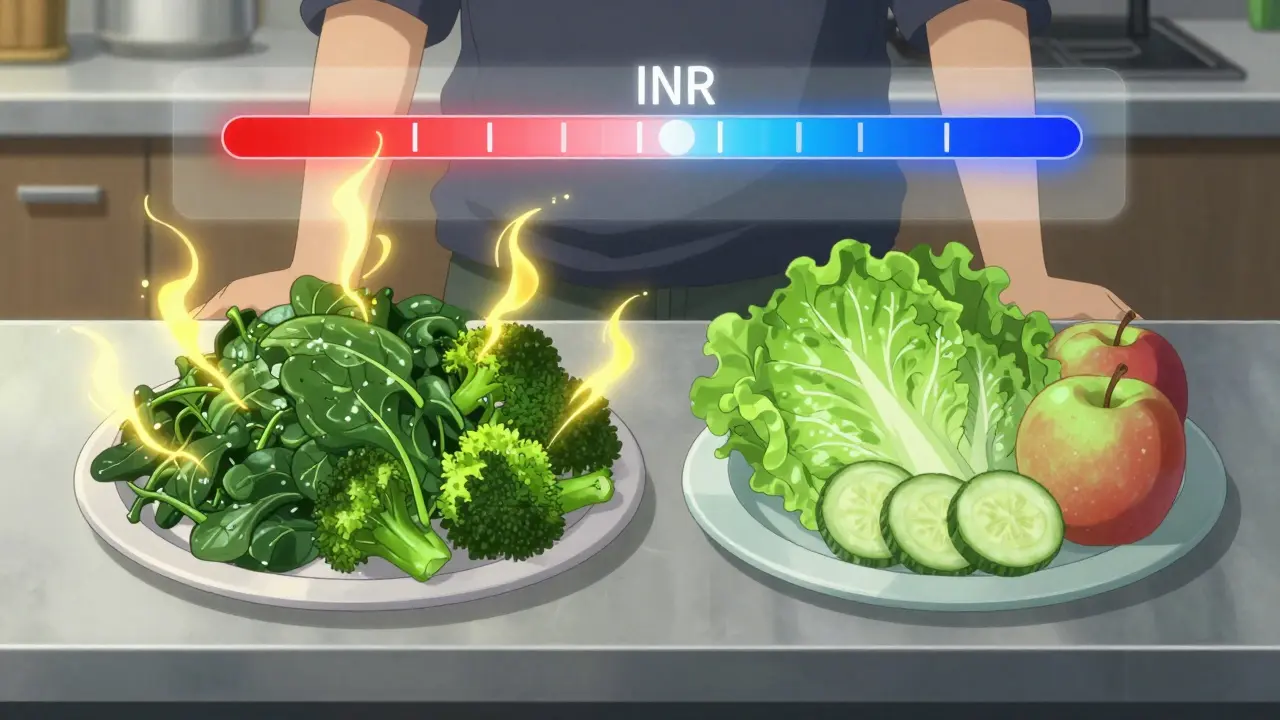
Warfarin doesn't make your blood thinner by thinning it out. It blocks a key step in the clotting process. Your liver needs vitamin K to activate clotting factors-proteins like II, VII, IX, and X-that help your blood form clots when you get cut. Warfarin shuts down the enzyme that recycles vitamin K, so those clotting factors can't do their job. That's how it prevents dangerous clots. But here's the catch: vitamin K from food fights back. Every time you eat spinach, kale, or broccoli, you're giving your liver a fresh supply of vitamin K. If you eat a lot one day and almost none the next, your body gets mixed signals. Warfarin is trying to slow clotting, but vitamin K is telling your liver to make more clotting factors. That’s why your INR jumps up and down.What Foods Have the Most Vitamin K?
Not all foods are equal when it comes to vitamin K. The American Heart Association says anything with more than 60 mcg per serving is a high-vitamin K food. These are the ones you need to watch:- Raw kale: 547 mcg per cup
- Cooked spinach: 889 mcg per cup
- Cooked broccoli: 220 mcg per cup
- Collard greens: 418 mcg per cup
- Swiss chard: 298 mcg per cup
- Brussels sprouts: 219 mcg per cup
- Parsley: 246 mcg per cup (just a few tablespoons)
What About Low-Vitamin K Foods?
Yes, there are plenty of foods that won’t mess with your INR. The American Heart Association calls these "Original Superfoods"-those with less than 35 mcg per serving. These are safe to eat freely:- Iceberg lettuce: 17 mcg per cup
- Cucumbers: 11 mcg per cup
- Carrots: 15 mcg per cup
- Apples: 5 mcg per medium fruit
- White rice: 3 mcg per cup cooked
- Eggs: 0.3 mcg per large egg
- Chicken breast: 0.5 mcg per 3 oz
Why Consistency Beats Restriction
For years, doctors told patients on warfarin to avoid vitamin K entirely. That advice has changed. The 2023 American College of Chest Physicians Guidelines now say: Don’t restrict. Just stabilize. Why? Because studies show that people who eat a consistent amount of vitamin K every day have better INR control than those who eat very little. One study in the Journal of Thrombosis and Haemostasis found that patients who ate exactly 1 cup of cooked broccoli daily for six months hit a 92% time in therapeutic range (TTR). That’s nearly perfect control. On the flip side, 68% of INR instability events are tied to sudden dietary changes. A Reddit user reported their INR dropped from 2.8 to 1.9 after eating one large kale smoothie. Another saw their INR spike to 4.1 after switching from spinach to iceberg lettuce. These aren’t rare stories-they’re common. The goal isn’t to eat zero vitamin K. It’s to eat the same amount every day. Within 10-15% variation. That’s it.How to Track Your Vitamin K Intake
You can’t eyeball this. A cup of cooked spinach isn’t the same as a handful of raw. Cooking, chopping, and even storage change vitamin K content. Here’s how to get it right:- Use a food tracking app like CoumaDiet (rated 4.6/5 by over 1,200 users). It’s built specifically for warfarin patients.
- Measure portions. Don’t guess. Use a measuring cup for greens, a food scale for cooked veggies.
- Log everything. Even a side of steamed broccoli counts.
- Plan meals ahead. If you know you’re having broccoli on Tuesday, make sure you have the same amount on Thursday and Saturday.
- Be consistent with cooking methods. Steaming preserves more vitamin K than boiling. Boiling can cut vitamin K by up to half.
What About Supplements and Fortified Foods?
Some patients struggle to keep intake stable. Maybe they travel often. Maybe they hate vegetables. The Anticoagulation Forum now recommends a daily low-dose vitamin K supplement-100-200 mcg-for those with erratic diets. Why? Because a 2022 study in Blood Advances found that taking 150 mcg of vitamin K daily actually reduced INR variability by 28%. It sounds backwards, but it works. If your intake is all over the place, giving your body a steady, predictable dose helps it adjust. Also, watch out for fortified foods. Some cereals, meal replacement shakes, and protein bars now add vitamin K. Check labels. A single bar might have 100 mcg-enough to throw off your INR if you’re not expecting it.What to Do When Your INR Goes Off Track
If your INR drops too low (below 2.0), you’re at risk for clots. If it spikes too high (above 4.0), you’re at risk for bleeding. Here’s what to do:- INR too low? Did you eat more vitamin K than usual? Cut back for a few days. Talk to your provider about a small dose increase.
- INR too high? Did you eat less vitamin K? Eat a consistent, moderate amount for the next few days. Your provider may lower your warfarin dose.
- Never change your dose yourself. Always consult your anticoagulation clinic or doctor.

When to Call Your Doctor
You don’t need to panic every time your INR moves a little. But here are red flags:- Your INR changes by more than 0.5 from your last reading without a clear reason.
- You’ve changed your diet in the last 3-5 days.
- You’re vomiting, have black stools, or notice unusual bruising.
- You’re starting a new medication (even over-the-counter ones like ibuprofen or antibiotics).
Real-Life Success Stories
One man in Ohio switched from eating random greens to eating exactly 1 cup of steamed broccoli every day. His TTR went from 45% to 89% in 10 weeks. He stopped getting emergency INR checks. A woman in Texas used to eat a big spinach salad every other day. Her INR bounced between 1.8 and 4.5. After switching to 1/2 cup of romaine daily and adding a 150 mcg vitamin K tablet, her INR stabilized at 2.6. She now travels without fear. These aren’t miracles. They’re simple, repeatable habits.Final Takeaway
You don’t need to be a nutrition expert. You don’t need to count every microgram. But you do need to be consistent. Eat about the same amount of vitamin K every day. Use a tracker. Measure your food. Avoid sudden changes. Your INR will thank you.Warfarin isn’t going away. Even with newer blood thinners, it’s still the only option for mechanical heart valves and antiphospholipid syndrome. That means for millions of people, vitamin K management isn’t optional-it’s essential. And the best part? You already have everything you need to get it right.
Can I eat leafy greens while on warfarin?
Yes, but you must eat the same amount every day. A cup of spinach one day and none the next will cause your INR to swing. Choose one or two consistent sources of vitamin K and stick to them. If you love kale, eat the same portion daily. If you prefer broccoli, do the same. Consistency is the key.
Does cooking affect vitamin K levels?
Yes. Boiling vegetables like spinach or broccoli can reduce vitamin K content by 30-50%. Steaming, sautéing, or eating raw preserves more. If you’re trying to keep intake stable, use the same cooking method every time. For example, if you steam your broccoli, keep steaming it-not boiling.
Should I take a vitamin K supplement?
For some people, yes. If your diet is inconsistent and your INR keeps fluctuating, a daily 100-200 mcg supplement can help stabilize things. Studies show it reduces variability. But never start a supplement without talking to your doctor first. It’s not a one-size-fits-all fix.
Can I drink alcohol while on warfarin?
Moderate alcohol (one drink per day) is usually fine, but heavy drinking can raise your INR and increase bleeding risk. Alcohol affects how your liver processes warfarin. If you drink regularly, keep your intake consistent. If you binge once a week, your INR will likely spike. Stick to small, steady amounts.
Why do some people say vitamin K doesn’t matter anymore?
Some studies, especially those that account for genetics, show vitamin K intake has less impact on warfarin dose than we once thought. But those studies look at average doses in large groups. For individual patients, dietary changes are still the #1 cause of INR instability. Even if genetics explain part of the variation, your daily food choices still matter most in real life.
How often should I get my INR checked?
Once a month is standard once you’re stable. But if your diet changes, you start a new medication, or your INR moves more than 0.5, check it sooner. Many clinics offer home testing kits-ask if that’s an option. More frequent monitoring means faster fixes.





Darren Torpey
March 5, 2026 AT 20:46My trick? I eat 1/2 cup steamed broccoli every single night. No exceptions. Weekends? Holidays? Still broccoli. My INR hasn't budged in over a year. You don't need to be perfect. You just need to be predictable.
Milad Jawabra
March 6, 2026 AT 21:12I had a 72-year-old man who was in the ER every 3 weeks because he'd eat a giant spinach salad on Sunday and then nothing all week. We switched him to 1 cup of steamed kale every Tuesday and Thursday. INR stable. No more ER trips.
Stop overcomplicating it. Your liver doesn't care about your #wellnessgoals. It just wants consistency.
Jane Ryan Ryder
March 7, 2026 AT 00:00Megan Nayak
March 8, 2026 AT 10:18Genetics explain 30-40% of variability. CYP2C9 and VKORC1 polymorphisms are well-documented. Yet here we are, blaming your salad.
Also, why is parsley on the list? It's a garnish. You're not eating 246 mcg of vitamin K in a sprinkle. This is nutritional pseudoscience dressed up as clinical advice.
Divya Mallick
March 9, 2026 AT 23:42You don't need apps. You don't need scales. You need routine. Your body isn't a lab. It's a rhythm.
Stop overthinking. Eat what you eat. Every. Single. Day.
And if you're eating kale smoothies? You're doing it wrong. Stop trying to be trendy. Your blood doesn't care about Instagram.
Alex Brad
March 10, 2026 AT 10:56Chris Beckman
March 12, 2026 AT 10:50Wait so I can eat spinach but only if I eat the same amount every day? But what if I like spinach on Monday and broccoli on Wednesday? Do I have to pick one?
Also I saw a guy on TikTok say vitamin K doesn't matter at all and he's still alive.
And why is iceburg lettuce on the list? That's basically water. Is that even food?
RacRac Rachel
March 14, 2026 AT 09:36I used to eat kale salads every other day. My INR was all over the place. I cried in the clinic. My nurse looked at me like I was a toddler.
Then I started eating 1/2 cup of steamed broccoli every single night. No exceptions. Even on my birthday.
My TTR went from 42% to 87% in 8 weeks. I haven't had a single bleed. I'm even traveling now.
Thank you for writing this. I finally feel like I'm not at war with my own body. 🙏❤️
Lebogang kekana
March 15, 2026 AT 06:22Every weekend I’d have a giant kale smoothie with spirulina and chia seeds. My INR would crash to 1.4. I thought I was being healthy. I was being a dumbass.
I switched to 1 cup of steamed broccoli every day. No more smoothies. No more 'detoxes'.
My INR is now rock solid at 2.5. I’m alive. I’m stable. I’m not dying.
TO EVERYONE OUT THERE: STOP TRYING TO BE A HEALTH INFLUENCER. JUST EAT THE BROCCOLI. 🥦✊
Callum Duffy
March 15, 2026 AT 15:18It is worth noting that the variability in vitamin K content between different cooking methods and food sources is often underestimated. A patient who believes they are consuming 'a serving' of spinach may, in fact, be consuming anywhere from 200 to 900 mcg depending on preparation.
Measurement tools, while inconvenient, are not optional for long-term safety.
Pankaj Gupta
March 17, 2026 AT 00:55Also, the claim that '68% of INR instability events are tied to dietary changes' needs a citation. The referenced study in JTH doesn't state that exact percentage.
These are small errors, but for a post that's meant to be life-saving, precision matters.
Levi Viloria
March 17, 2026 AT 05:49So I kept eating my salsa verde and guacamole. I just stopped eating the kale.
My INR didn't change. My taste did.
Point is: you don't have to give up your culture. Just know what's in it. And keep it steady.
Renee Jackson
March 17, 2026 AT 07:07Patients who are able to integrate stable vitamin K intake into their existing dietary patterns demonstrate significantly improved adherence and reduced anxiety.
I will be sharing this resource with my entire anticoagulation clinic. Your work here is exemplary.