Quick Summary
- End‑stage Liver Failure is a life‑threatening condition that often requires a transplant.
- Liver Transplant replaces the diseased organ with a healthy donor liver.
- Two donor pathways exist - living donor and deceased donor - each with distinct risks and waiting times.
- Eligibility hinges on the MELD score, transplant centre assessment, and organ‑allocation rules.
- Post‑surgery survival exceeds 80% at five years when immunosuppression is managed properly.
Understanding End‑Stage Liver Failure
Liver Failure is a condition where the liver can no longer perform its essential metabolic, synthetic and detoxifying functions. Common causes include chronic hepatitis C, alcoholic liver disease, non‑alcoholic steatohepatitis (NASH) and genetic disorders such as Wilson’s disease. In the United Kingdom, roughly 1,600 patients are listed for a liver transplant each year, and mortality without transplantation rises sharply after a MELD (Model for End‑Stage Liver Disease) score of 15.
The liver’s inability to clear toxins leads to jaundice, ascites, hepatic encephalopathy and bleeding tendencies. When medical therapy fails, the only curative option is organ replacement.
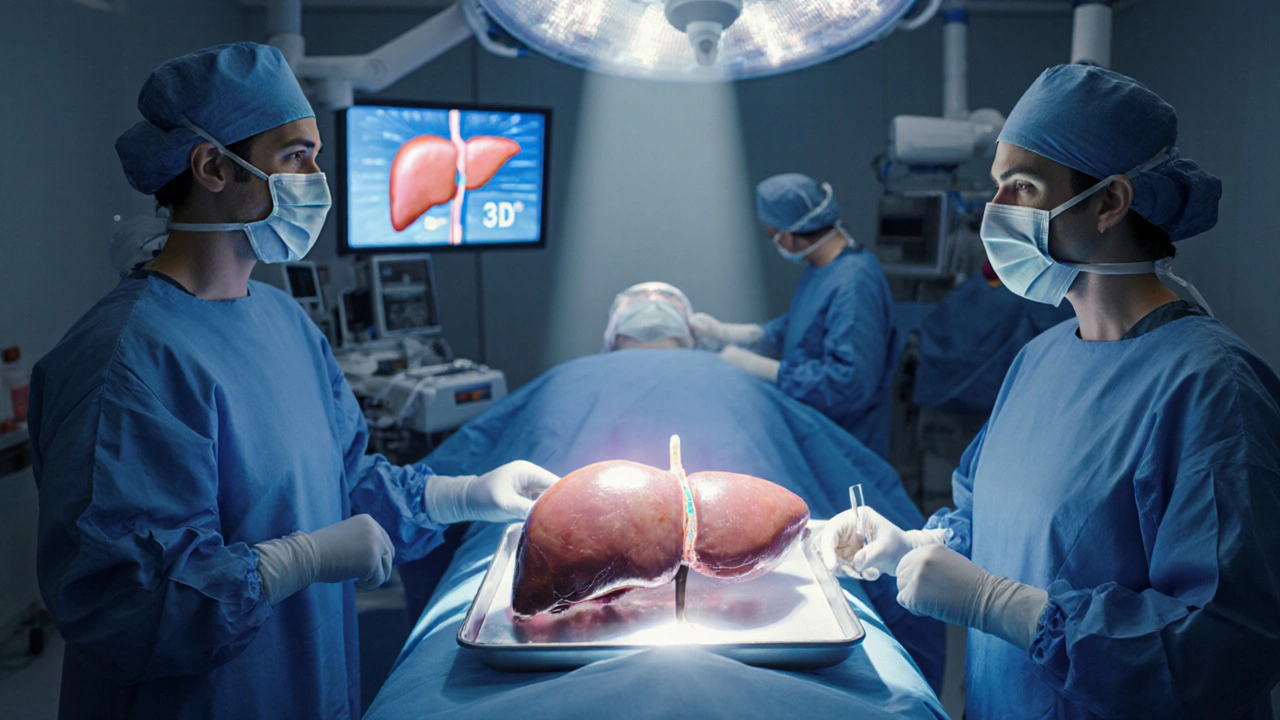
What Is a Liver Transplant?
Liver Transplant is a surgical procedure that removes a diseased liver and replaces it with a healthy donor graft. The operation typically lasts 6-10hours and requires a multidisciplinary team: transplant surgeons, hepatologists, anesthesiologists, and transplant coordinators. According to the British Transplant Society, 5‑year survival after a first‑time transplant now exceeds 80% in high‑volume centres.
The graft can come from a living donor - usually a relative who donates a portion of their liver - or from a deceased donor whose organ becomes available through the national allocation system.
Types of Liver Donation
Choosing between a living donor and a deceased donor hinges on medical urgency, donor availability and patient preference. Below is a side‑by‑side comparison.
| Attribute | Living Donor | Deceased Donor |
|---|---|---|
| Source | Living Donor - a healthy relative or friend | Deceased Donor - organ recovered after brain death |
| Waiting Time | Weeks to months (planned) | Variable, often several months to years |
| Graft Survival (5‑yr) | ~90% | ~80% |
| Recipient Risks | Higher early‑post‑op complications due to smaller graft volume | Risk of organ‑cold‑ischemia injury |
| Donor Risks | Major abdominal surgery; 0.1‑0.5% serious complication rate | None (donor is deceased) |

Evaluating Candidates for Transplant
The first step is an objective assessment of disease severity. The MELD Score is a numeric scale (6‑40) that predicts three‑month mortality based on bilirubin, INR and creatinine. A score above 15 typically triggers placement on the national waiting list.
Patients are then referred to a Transplant Center, which conducts a comprehensive evaluation - cardiac work‑up, infection screening, psychosocial assessment and imaging studies. Only centres accredited by NHS Blood and Transplant can list patients for organ allocation.
The organ allocation system prioritises based on MELD, blood type compatibility, donor‑recipient size match, and geographical proximity to minimise cold‑ischemia time. Patients with acute liver failure or hepatocellular carcinoma receive special exception points.
Surgery and Immediate Post‑Operative Care
During the operation, the recipient’s diseased liver is removed and the donor graft is implanted. Vascular anastomoses (hepatic artery, portal vein, hepatic veins) and bile duct reconstruction are the most technically demanding steps.
After surgery, patients enter an intensive‑care unit for close monitoring of graft function, blood flow, and signs of rejection. Immunosuppression therapy, typically a combination of tacrolimus, mycophenolate mofetil and steroids, is started immediately to prevent immune‑mediated graft injury. Blood levels are adjusted daily during the first two weeks, then tapered over months.
Complications can include vascular thrombosis, biliary leaks, infection and acute rejection. Early detection via Doppler ultrasound and liver function tests is crucial.
Long‑Term Outcomes and Quality of Life
When immunosuppression is well‑controlled, most recipients enjoy a dramatic improvement in quality of life. Studies from the European Liver Transplant Registry report a 5‑year Post‑Transplant Survival rate of 82% for adults and 85% for pediatric patients.
Long‑term risks include chronic kidney disease, metabolic syndrome, and malignancies linked to lifelong immunosuppression. Lifestyle modifications-balanced diet, regular exercise, abstaining from alcohol-are strongly advised.
Follow‑up care involves quarterly liver function tests for the first year, then bi‑annual monitoring. Patients remain on low‑dose immunosuppression indefinitely, but many centres are exploring protocol‑driven withdrawal for low‑risk individuals.
Related Topics to Explore
- Management of portal hypertension before transplant.
- Living donor evaluation and ethical considerations.
- Advances in normothermic machine perfusion for organ preservation.
- Psychological support for transplant candidates and families.
- Future of regenerative medicine: bio‑engineered livers.
Frequently Asked Questions
How long does a liver transplant surgery take?
The operation usually lasts between six and ten hours, depending on whether the graft is from a living or deceased donor and on the recipient’s anatomy.
What is the typical waiting time for a deceased‑donor liver?
Waiting time varies widely but averages 9‑12 months in the UK. Urgency, blood type, and MELD score can shorten or lengthen this period.
Can a living donor donate a portion of their liver safely?
Yes. The donor’s remaining liver regenerates to near‑normal size within 6‑8 weeks. Serious complications occur in less than 0.5% of donors.
What are the main side effects of immunosuppressive drugs?
Common side effects include increased infection risk, high blood pressure, kidney dysfunction, tremor, and weight gain. Regular monitoring helps mitigate these risks.
How is graft function monitored after surgery?
Doctors track liver enzymes (ALT, AST), bilirubin, INR, and imaging studies such as Doppler ultrasound to ensure adequate blood flow and early detection of rejection.
Is a second liver transplant ever needed?
Yes. About 10‑15% of recipients may require retransplantation due to chronic rejection, recurrent disease, or graft failure.
How does alcohol consumption affect post‑transplant outcomes?
Continued heavy drinking dramatically raises the risk of graft loss and mortality. Most centres require a six‑month abstinence period before listing.
What lifestyle changes are recommended after a liver transplant?
Patients should follow a balanced low‑sodium diet, maintain a healthy weight, avoid alcohol, stay up‑to‑date with vaccinations, and attend regular clinic appointments.






Kerri Burden
September 27, 2025 AT 14:08The distinction between living‑donor and deceased‑donor grafts hinges on donor logistics and graft viability metrics. A living donor typically offers a segment that regenerates, which shortens cold‑ischemia time and preserves endothelial function. Deceased donors, while more readily available, introduce variability in donor‑recipient size matching and potential ischemic injury. Moreover, the post‑transplant immunosuppression regimen must be calibrated to the graft type to mitigate rejection risk without over‑suppressing immunity. All of these factors feed into a nuanced risk‑benefit analysis that transplant teams evaluate case‑by‑case.
Joanne Clark
October 2, 2025 AT 00:25Honestly, the whole graft allocation paradigm is just a glorified lottery, lol.
George Kata
October 6, 2025 AT 10:41When assessing a candidate for liver transplantation, the multidisciplinary team initiates a comprehensive work‑up that begins with a precise calculation of the MELD score, which quantifies mortality risk based on bilirubin, INR, and creatinine levels. Following this quantification, the patient undergoes cardiac evaluation, infectious disease screening, and psychosocial assessment to ensure both physiological readiness and post‑operative compliance. The allocation algorithm then cross‑references blood type compatibility, donor‑recipient size ratios, and geographic proximity to minimize cold‑ischemia duration, an essential factor for graft survivability. Living‑donor transplantation offers the advantage of elective scheduling, thereby allowing pre‑emptive optimization of the recipient’s nutritional status and metabolic parameters. Conversely, deceased‑donor grafts, while less predictable in timing, benefit from the opportunity to select organs with optimal perfusion metrics, often resulting in comparable long‑term graft function. Immunosuppressive protocols, typically anchored by tacrolimus, are individualized based on trough levels, renal function, and the presence of comorbidities such as diabetes or hypertension. Early postoperative monitoring incorporates Doppler ultrasonography to assess hepatic arterial flow, and serial liver function tests to detect biochemical signs of rejection. Should acute rejection be identified, the therapeutic cascade may include pulse steroids, anti‑lymphocyte globulin, or modulation of calcineurin inhibitor dosing. Finally, the longitudinal follow‑up strategy emphasizes renal preservation, metabolic syndrome mitigation, and vigilant surveillance for de‑novo malignancies, all of which are paramount in sustaining the remarkable five‑year survival rates reported in high‑volume centers.
Nick Moore
October 10, 2025 AT 20:58It's pretty awesome how the survival rates have climbed above 80% at five years – that’s a huge win for the field. The surgical teams have gotten slick with those 6‑10 hour operations, and the anesthesiologists keep everything steady. Plus, the fact that living donors can bounce back so quickly is just mind‑blowing. If you’re on the list, staying positive and following the clinic’s advice can make a big difference in outcomes. Remember, the meds might make you gain a few pounds, but they’re keeping the graft alive.
Jeffery Reynolds
October 15, 2025 AT 07:15The immunosuppressive regimen must be titrated with surgical precision; any deviation can precipitate graft rejection or opportunistic infection. Patients should adhere to scheduled lab draws, as tacrolimus levels dictate dose adjustments. Moreover, the protocol mandates low‑dose steroids only during the initial post‑operative window to minimize systemic side‑effects. It is also essential to monitor renal function vigilantly due to nephrotoxic potential of calcineurin inhibitors. Finally, lifestyle modifications, including a low‑sodium diet, bolster long‑term graft health.
Mitali Haldankar
October 19, 2025 AT 17:31Wow, liver transplants are truly a miracle, but honestly, I wonder why we don’t push for artificial livers more 😏. The donor shortage is real, yet the tech is there, kinda. 🤔 Anyway, if you’re lucky enough to get a donor, cherish that second chance! 🎉
snigdha rani
October 24, 2025 AT 03:48Oh great, another post about how awesome liver transplants are. As if we didn’t already know the meds make you gain weight. And sure, the graft survival is “90%,” but that’s only if you follow the strict diet. I guess good luck with the endless blood tests, right?
Mike Privert
October 28, 2025 AT 13:05For anyone on the waiting list, keep focusing on the things you can control: nutrition, staying active, and sticking to your medication schedule. Your transplant team will monitor labs and adjust doses, so trust the process. If you feel overwhelmed, reach out to support groups – sharing experiences helps a lot. Remember, each small step today adds up to a healthier post‑transplant life tomorrow.
Veronica Lucia
November 1, 2025 AT 23:21One might contemplate the philosophical implications of receiving another's organ – an intimate intertwining of lives. Yet, the practical reality underscores the resilience of the human body when aided by science. The transplant journey becomes a meditation on mortality and hope. Ultimately, the graft serves as a reminder of our collective interdependence.
Sriram Musk
November 6, 2025 AT 09:38From a clinical standpoint, the pre‑transplant evaluation must satisfy stringent criteria, including cardiac clearance and infection screening. Donor‑recipient ABO compatibility remains a non‑negotiable parameter to prevent hyperacute rejection. The surgical technique demands precise vascular anastomosis to ensure graft perfusion. Post‑operatively, tacrolimus trough levels are monitored daily until stabilization. Regular follow‑up appointments are essential for long‑term graft surveillance.
allison hill
November 10, 2025 AT 19:55Everyone acts like liver transplants are the ultimate cure, but have they considered the hidden agenda of pharmaceutical companies? It's all about profit, not patients. The media paints it as a miracle, yet the side‑effects are downplayed. Trust me, there’s more to the story than they let on. Stay vigilant, question everything.
Tushar Agarwal
November 15, 2025 AT 06:11Hey folks! Just wanted to say that the post‑transplant care routine isn’t as scary as it seems 😊. Keep up with your meds, attend your appointments, and you’ll do fine. If you ever feel unsure, don’t hesitate to ask your nurse – they’re there to help! 👍
Julia Gonchar
November 19, 2025 AT 16:28Let’s break it down: the MELD score is calculated using bilirubin, INR, and creatinine – that’s basic math. Living donors cut down wait time dramatically, but they take on surgical risk, however small. Deceased donors are unpredictable, but the grafts are whole, which some surgeons prefer. Immunosuppression protocols vary, but tacrolimus remains the backbone. Bottom line: it’s a balance of risk, timing, and logistics.
Annie Crumbaugh
November 24, 2025 AT 02:45Liver transplants save lives, but you have to follow the doctor’s orders. Take your meds, eat healthy, and go to appointments. That’s it.