Your kidneys are hard workers. Every day, they filter about 180 liters of blood to remove waste and balance fluids. But what happens when your body’s own defense system turns against these filters? That is exactly what occurs in glomerulonephritis, a condition where the immune system mistakenly attacks the glomeruli-the microscopic filtering units of the kidneys. It is not just one disease; it is a group of disorders that share this common mechanism of immune-mediated damage. If left unchecked, this inflammation can scar the delicate filtration barrier, leading to permanent kidney failure.
The good news is that we understand more about this condition than ever before. We know why it happens, how to spot the early warning signs, and-crucially-we have new treatments that target the root cause rather than just suppressing the entire immune system. This guide breaks down the complex biology of glomerulonephritis into plain language so you can understand what is happening inside your body and what options exist for care.
How the Kidney Filter Works (and How It Breaks)
To understand glomerulonephritis, you first need to visualize the glomerulus. Think of it as a high-tech coffee filter, but billions of times smaller and far more selective. Inside each kidney, there are about one million of these tiny clusters of capillaries called glomeruli. Their job is to let waste and excess fluid pass through into the urine while keeping essential proteins and blood cells in the bloodstream.
This filtration barrier relies on three critical components working in harmony:
- The endothelial glycocalyx and glomerular endothelial cells: These line the inside of the capillaries and act as the first layer of defense.
- The glomerular basement membrane (GBM): A thick, tough sheet that acts as the main structural filter.
- The podocytes (visceral epithelial cells): Specialized cells with finger-like projections that wrap around the GBM. They are the final checkpoint, ensuring only waste passes through.
In glomerulonephritis, the immune system identifies parts of this structure as foreign threats. It sends antibodies or immune complexes to attack them. This causes swelling, scarring, and leakage. When the podocytes are damaged, they lose their ability to hold back protein. The result is proteinuria-protein leaking into the urine-which is often the first sign that something is wrong.
Spotting the Signs: Nephritic vs. Nephrotic Syndromes
Glomerulonephritis does not always announce itself with pain. In fact, many people feel fine until routine blood or urine tests reveal abnormalities. When symptoms do appear, they usually fall into two distinct patterns known as syndromes. Recognizing which pattern you have helps doctors determine the severity and type of GN.
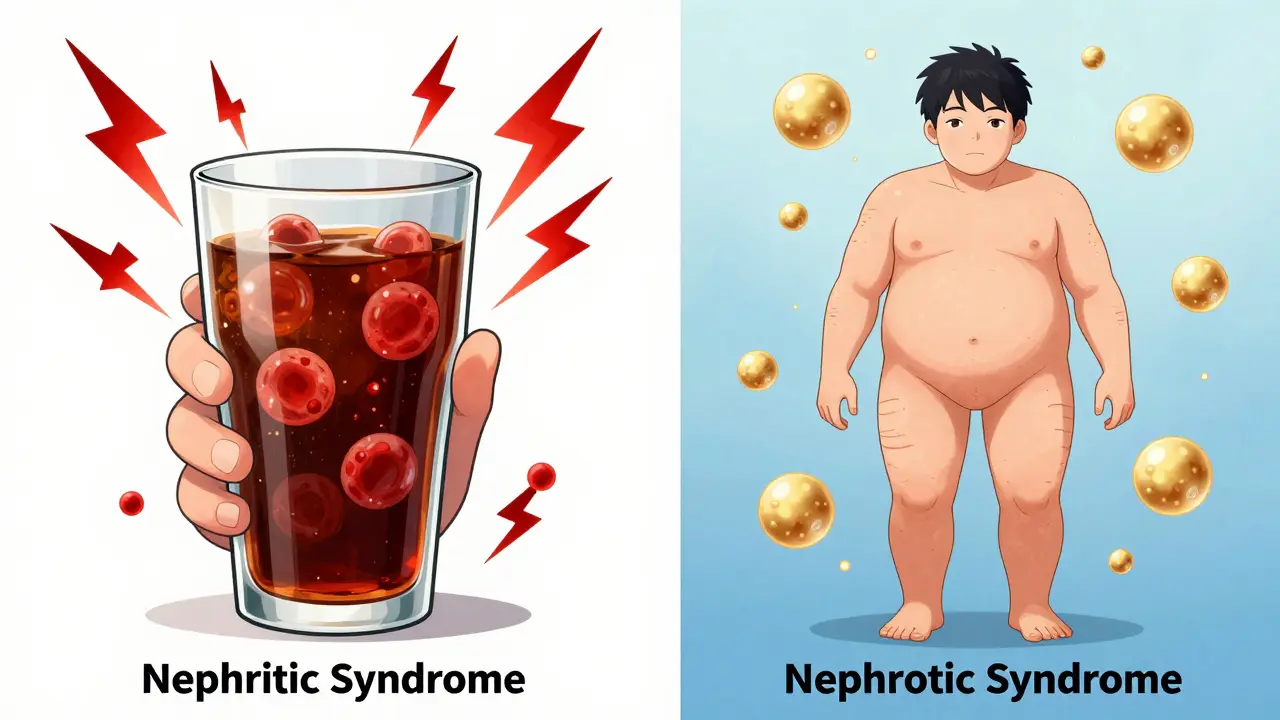
Nephritic Syndrome is characterized by active inflammation. You might notice blood in your urine (hematuria), which can make it look pink, red, or cola-colored. High blood pressure is common because the kidneys struggle to regulate fluid volume. You may also experience mild swelling in the face or ankles and a slight reduction in kidney function, often seen as elevated serum creatinine levels (typically between 1.5-3.0 mg/dL).
Nephrotic Syndrome indicates more severe damage to the filtration barrier. The hallmark here is massive protein loss. If you excrete more than 3.5 grams of protein per day, you likely have nephrotic-range proteinuria. This leads to low albumin levels in the blood (hypoalbuminemia below 3.0 g/dL), which causes fluid to leak out of blood vessels into tissues, resulting in significant edema (swelling) in the legs, abdomen, and even lungs. Patients often develop high cholesterol (hyperlipidemia) as the liver tries to compensate for the lost proteins.
Types of Glomerulonephritis: Why Classification Matters
Not all glomerulonephritis is the same. The treatment depends heavily on the underlying cause. Doctors classify GN based on how the immune system triggers the attack. Here are the most common types:
| Type | Cause/Mechanism | Key Feature | Prognosis |
|---|---|---|---|
| IgA Nephropathy | Deposition of IgA antibodies in glomeruli | Most common primary GN worldwide; often follows respiratory infections | 20-40% progress to end-stage renal disease over 20 years |
| Lupus Nephritis | Autoimmune reaction from Systemic Lupus Erythematosus (SLE) | Affects 50-60% of SLE patients; involves multiple organ systems | 70-80% 10-year renal survival with current treatments |
| Post-Streptococcal GN | Immune response to strep throat or skin infection | Common in children; acute onset | 95% recovery within 6-8 weeks |
| C3 Glomerulonephritis (C3G) | Dysregulation of the complement system (C3 protein) | C3 protein accumulates in glomeruli at 3-5x normal levels | Variable; requires targeted therapy to prevent progression |
| Membranoproliferative GN (MPGN) | Immune complex deposition or complement dysregulation | Thickened basement membrane; reduced kidney function | 50-60% 10-year survival without treatment; better with intervention |
For example, IgA Nephropathy (also known as Berger’s disease) is the most common form globally. It often strikes young adults after a cold or flu, causing temporary blood in the urine. In contrast, C3 Glomerulonephritis is rarer and driven by a malfunction in the complement system-a part of the immune system meant to help clear bacteria. In C3G, this system gets stuck in the "on" position, constantly attacking the kidneys.
The Diagnostic Journey: Biopsy and Beyond
You cannot diagnose glomerulonephritis with a simple blood test. While blood work can show elevated creatinine or abnormal protein levels, it cannot tell you *why* the kidneys are failing. The gold standard for diagnosis is a kidney biopsy.
During this procedure, a nephrologist uses a needle to take a tiny sample of kidney tissue. This sounds scary, but it is generally safe, with a complication rate of only 3-5% (mostly minor bleeding). The tissue is then examined under a microscope by a nephropathologist-a specialist who has spent 5-7 years training specifically to read these complex patterns.
The biopsy reveals the specific type of GN by showing where immune deposits are located and how much scarring has occurred. Recent advances allow doctors to use molecular biomarkers alongside traditional histology. According to the European Renal Association’s 2023 guidelines, this combined approach predicts treatment response with 85% accuracy, compared to just 65% with histology alone.
Treatment Options: From Steroids to Targeted Therapies
Treating glomerulonephritis is a balancing act. You need to stop the immune attack without weakening the body so much that it becomes vulnerable to infections. For decades, the go-to treatment was corticosteroids (like prednisone). They work fast, reducing inflammation in 60-80% of patients. However, they come with heavy costs: weight gain (reported by 72% of patients), increased infection risk, bone density loss, and mood swings.
We are now entering a new era of targeted therapies. Instead of blanketing the whole immune system, these drugs aim at specific pathways involved in GN.
- Eculizumab: A monoclonal antibody that blocks the complement system. It has shown promise in C3G, reducing proteinuria by 40-50% at 12 months. However, it is expensive, costing approximately $500,000 annually.
- Iptacopan: Recently granted breakthrough therapy designation by the FDA for C3G. Phase II trials showed a 52% reduction in proteinuria compared to placebo. It works by inhibiting a specific enzyme in the complement cascade.
- Rituximab: Often used for lupus nephritis and other autoimmune-related GN. It depletes B-cells, which produce the harmful antibodies. Many patients report that starting rituximab early prevented the need for dialysis.
The KDIGO (Kidney Disease: Improving Global Outcomes) 2023 guidelines recommend a minimum 6-month trial of standard therapy before switching to novel agents. Regular monitoring is crucial: serum creatinine should be checked every two weeks initially, and proteinuria monthly. This close watch allows doctors to adjust doses quickly if side effects arise or if the disease flares up.

Living with Glomerulonephritis: Managing Symptoms and Stress
A diagnosis of GN can be overwhelming. Patient surveys indicate that 65% of GN patients experience significant fatigue, with nearly half citing it as their most debilitating symptom. Edema (swelling) is another major challenge, mentioned in 78% of patient forum posts. Managing this often involves strict sodium restriction and diuretic medications.
Mental health is just as important as physical health. Anxiety about disease progression affects 51% of patients. Joining support groups, whether online communities like Inspire.com or local chapters, can provide practical tips and emotional relief. Sharing experiences about medication side effects or diet adjustments can empower you to take control of your care.
Diet plays a huge role. Reducing salt intake helps manage blood pressure and swelling. Limiting protein intake may ease the workload on the kidneys, though this should be done under a doctor’s supervision to avoid malnutrition. Staying hydrated is key, but fluid restrictions may be necessary if edema is severe.
The Future of GN Research
The landscape of glomerulonephritis treatment is changing rapidly. The global market for GN treatments is projected to grow from $2.3 billion in 2022 to $4.7 billion by 2028. This growth reflects both an increase in awareness and the development of new drugs.
Experts predict that within five years, genetic and proteomic profiling will guide personalized therapy selection. Imagine a future where your treatment plan is tailored to your specific genetic markers, increasing efficacy from the current 60-70% to over 85%. However, access remains a challenge. Patients in low-income countries have 70% less access to advanced diagnostics and 90% less access to novel therapeutics. Advocacy groups are working to bridge this gap, ensuring that life-saving treatments reach everyone who needs them.
Is glomerulonephritis curable?
It depends on the type. Post-streptococcal GN often resolves completely on its own within weeks. For chronic forms like IgA nephropathy or lupus nephritis, there is no outright cure, but the disease can often be put into remission with medication. Early detection and aggressive treatment can preserve kidney function for decades.
What foods should I avoid with glomerulonephritis?
The most important change is reducing sodium (salt) to control blood pressure and swelling. You may also need to limit potassium and phosphorus if your kidney function declines significantly. Processed foods, canned soups, and fast food are typically high in sodium and should be avoided. Always consult a renal dietitian for a personalized plan.
How long does a kidney biopsy take?
The actual procedure takes about 15-30 minutes. However, you will need to rest in bed for several hours afterward to prevent bleeding. Most patients go home the same day, but some stay overnight for observation. Results usually take 1-2 weeks as the tissue is processed and analyzed by a pathologist.
Can stress trigger glomerulonephritis?
Stress does not directly cause GN, but it can weaken the immune system and potentially trigger flares in existing autoimmune conditions like lupus. Managing stress through relaxation techniques, adequate sleep, and support networks is an important part of overall kidney health management.
What is the difference between nephritic and nephrotic syndrome?
Nephritic syndrome is marked by inflammation, blood in the urine, high blood pressure, and mild swelling. Nephrotic syndrome is characterized by massive protein loss in the urine, severe swelling (edema), low blood protein levels, and high cholesterol. Nephrotic syndrome generally indicates more severe damage to the filtration barrier.
Are new treatments like iptacopan covered by insurance?
Coverage varies widely by insurer and region. Because these drugs are expensive, manufacturers often offer patient assistance programs. Your nephrologist’s office staff can help navigate prior authorizations and financial aid options to reduce out-of-pocket costs.